
Table of contents
Blastocyst Formation
The first week post-fertilization is critically important for embryonic development. During this period, the embryo undergoes several complex processes, the outcomes of which significantly impact the success of embryo transfer and pregnancy. Within 7 days, the embryo must progress through the stages of pronuclei formation and fusion (the merging of the egg and sperm nuclei to form the zygote nucleus), cleavage, compaction, and blastocyst formation.

A blastocyst forms on days 5–7 of embryonic development and consists of 156–200 cells. It comprises a cavity (blastocoel) and two populations of pluripotent cells: the inner cell mass (ICM) and the trophectoderm (TE). The ICM develops into all types of embryonic cells, while the TE forms the placenta.
Classification and Selection of Blastocysts for Embryo Transfer
Blastocysts are classified internationally using the Gardner scale, which includes one number and two capital letters. The number denotes the size of the blastocyst cavity, the first letter represents the quality of the ICM, and the second letter indicates the quality of the TE. Under a microscope, embryologists assess the quality of blastocysts based on morphology.
Blastocyst size and blastocoel volume (1–6):
1. The cavity occupies <50% of the blastocyst.
2. The cavity occupies 50% of the blastocyst.
3. The cavity occupies >75% of the blastocyst.
4. The blastocyst cavity is twice the size of the ICM.
5. The blastocyst begins hatching from the zona pellucida.
6. The blastocyst is completely free from the zona pellucida and ready for implantation.

Fig. 1. Very early blastocyst with a small cavity in the center.
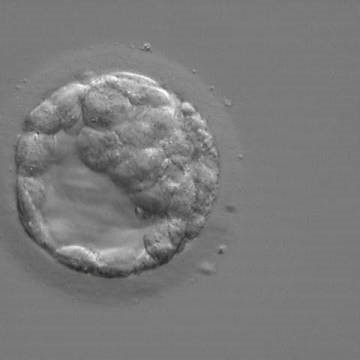
Fig. 2. Early blastocyst with a clearly visible cavity occupying half of the embryo’s volume.

Fig. 3. Blastocyst whose cavity occupies more than 50% of the embryo’s volume. The overall volume of the blastocyst remains unchanged without thinning of the zona pellucida (ZP). The early ICM can be seen in the upper part of this image.
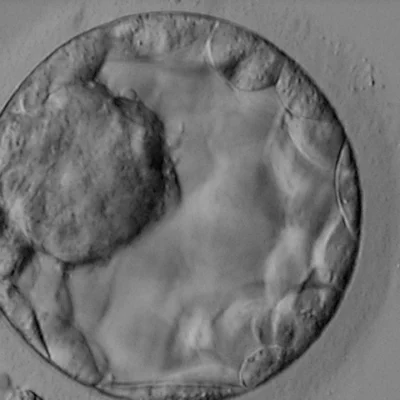
Fig. 4. Blastocyst with a cavity twice the size of the inner cell mass (ICM). The ICM consists of many tightly packed cells.
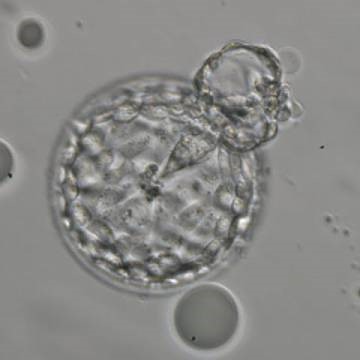
Fig. 5. Beginning of hatching in the blastocyst: a small triangular ICM emerges along with TE cells. The blastocyst cavity is lined by many TE cells of similar size, and the ZP is thinned.
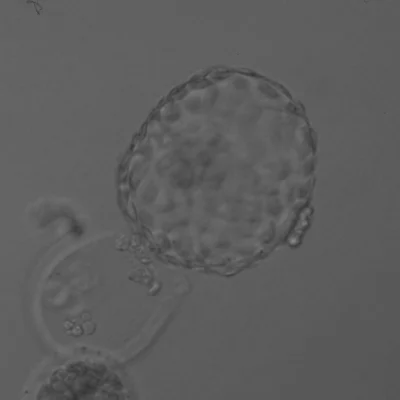
Fig. 6. Blastocyst after hatching, free from the zona pellucida (ZP). The ICM is slightly out of focus in this image and consists of many cells. The TE similarly consists of many cells forming a cohesive epithelium. Some cellular debris is expelled from the ZP.
Inner Cell Mass (ICM) Quality (future fetus) (7-10):
– A: Numerous cells with indistinct boundaries.
– B: Recognizable cell shapes with minor defects (fragmentation).
– C: Significant cellular defects and signs of apoptosis (cell death).
– D: Degenerated cells.

Fig. 7. Blastocyst (4AA) with a large ICM, consisting of many cells and well-compacted.
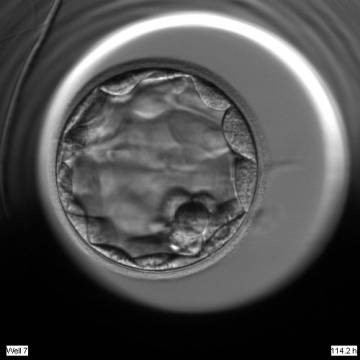
Fig. 8. Blastocyst (3BA) with a very small ICM, consisting of only a few cells.
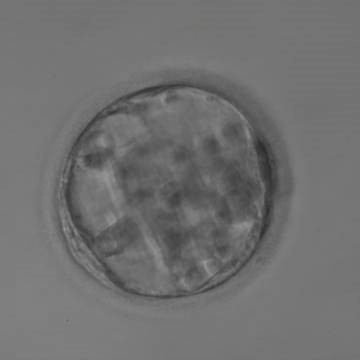
Fig. 9. Blastocyst (quality 3BB) without a clearly identifiable ICM and with a thin TE.
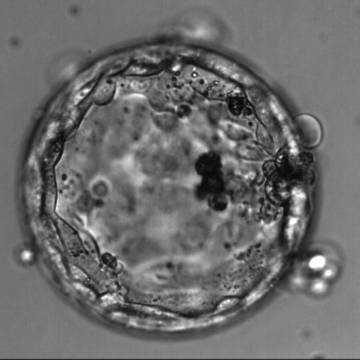
Fig. 10. Blastocyst beginning to hatch (4BA) without a clearly identifiable ICM, but with TE consisting of many cells forming a cohesive epithelium. Dark degenerating cells are present on the right side of the image.
Trophectoderm (TE) Quality (future placenta):
– A: Numerous cells forming a dense, uniform layer.
– B: Slightly reduced or unevenly distributed cell mass.
– C: Few cells with defects or inclusions.
– D: Degeneration processes present.
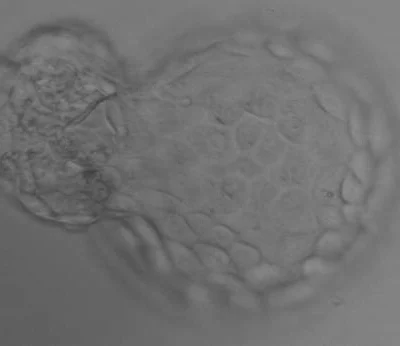
Fig. 11. Blastocyst beginning to emerge from the zona pellucida (5AA) with many cells forming the trophoectoderm (TE). The ICM is visible through a rupture in the ZP.

Fig. 12. Blastocyst (5AB) with a few TE cells forming a loosely connected epithelium and the ICM at the upper part of the image.

Fig. 13. Early hatching of the blastocyst (5AC) with very thin TE, where the cells do not form a cohesive epithelium. The ICM is well visualized at the upper left of the image.
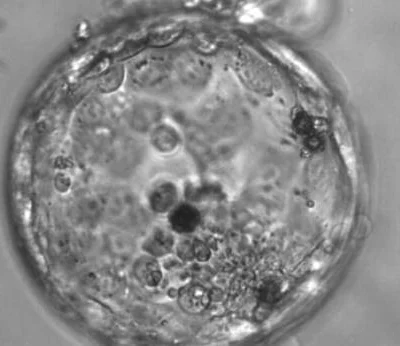
Fig. 14. Hatching of the blastocyst (5CC). TE cells vary in size and do not form a cohesive epithelium. A few loosely connected ICM cells can be seen at the bottom right of the image. Several dark degenerative areas are present inside the blastocyst.
Impact of Age and Embryo Morphology on Live Birth Rates Following Blastocyst Transfer Without Biopsy
High-quality blastocysts (AA/AB/BA) show significantly higher implantation and live birth rates than medium-quality (BB/CB) or poor-quality (BC/CC) blastocysts. Medium-quality blastocysts also have the potential for successful implantation and development. Poor-quality blastocysts, however, often lack sufficient energy reserves and are usually not considered for transfer.
Impact of Age and Embryo Morphology on Live Birth Rates
A 2015 study evaluated live birth outcomes in women aged 40–44 based on the number and quality of transferred blastocysts:
- 21.2% of “A” quality blastocysts led to live births (p < 0.0001).
- 10.5% of “B” quality blastocysts resulted in live births (p = 0.001).
- 5.6% of “C” quality blastocysts showed positive outcomes (p = 0.056).
- D-quality embryos contributed insignificantly (p = 0.71).
Among 80 transfers where the highest-quality embryos were morulas, only 3 children were born (3.8%). Interestingly, transferring at least one high-quality blastocyst significantly improved live birth rates. However, transferring multiple blastocysts, regardless of quality, increased the risk of multiple pregnancies.
In a 2021 study, TE morphology was identified as a better predictor of live birth rates than ICM morphology. For younger women (ages 25–32), live birth rates per single embryo transfer were:
- 51% for high-quality blastocysts (AA/AB/BA).
- 39% for medium-quality blastocysts (BB/CB).
- 25% for poor-quality blastocysts (BC/CC).
For older women (ages 40–44), the rates were:
- 22% for high-quality embryos.
- 14% for medium-quality embryos.
- 8% for poor-quality embryos.
Effect of Cryopreservation on Embryo Quality
Cryopreservation typically does not negatively affect embryo quality. Using vitrification and cryoprotectants protects embryonic cells during freezing by preventing ice crystal formation. However, some embryos may exhibit slightly lower quality after thawing. Re-freezing (re-cryopreservation) may be less beneficial for embryos.
Conclusions
Blastocyst quality is a crucial criterion for selecting embryos for transfer. High-quality blastocysts demonstrate significantly higher implantation and live birth rates compared to medium- or poor-quality blastocysts. However, medium-quality embryos still have the potential for successful outcomes.
Maternal age plays a decisive role in reducing implantation success, even for high-quality embryos, due to the increased risk of chromosomal abnormalities (aneuploidy). The Gardner classification evaluates morphology, but it may not always be sufficient for every case. For a more comprehensive assessment of embryo quality and to transfer chromosomally healthy (euploid) embryos, preimplantation genetic testing (PGT-A) may be recommended based on medical history.
References:
- Richter, K. S., O’Brien, J. E., Tucker, M. J., & Stillman, R. J. (2015). Blastocyst transfer in women aged 40 years or older: how many is too many? Fertility and Sterility, 104(3), e58. https://doi.org/10.1016/j.fertnstert.2015.07.175
- Awadalla, M., Kim, A., Vestal, N., Ho, J., & Bendikson, K. (2021). Effect of Age and Embryo Morphology on Live Birth Rate After Transfer of Unbiopsied Blastocysts. JBRA Assisted Reproduction, 25(3), 373. https://doi.org/10.5935/1518-0557.20200101
- https://atlas.eshre.eu/ – Atlas of human embryology.