Embryology
Classification of Oocytes
The Structure of Oocyte

Egg quality assessment
Egg quality is an important component of the success of an IVF program.
The morphology (appearance) of the egg is one of the ways in which we can assess its quality.
The ovum is 80,000 times larger than the sperm. This is due to the fact that it is the oocyte that transfers the entire supply of nutrients and energy for the subsequent development of the embryo.
The egg is surrounded by a membrane called the zona pellucida, which protects the egg and acts as a container for the embryo during its development until the implantation stage.
Further, the perivitelline space passes through the zone. This is the space between the zona pellucida and the oocyte itself.
Inside the oocyte is the cytoplasm, which contains many tiny cellular organs called organelles that are essential for the life of the egg.
The polar body is outside the oocyte at the 12 o’clock position, indicating that the oocyte is mature (ready for fertilization).
The egg nucleus contains genetic material (chromosomes and DNA).
Embryologists can assess the quality of oocytes by the appearance of the cytoplasm, the state of the vitelline layer and the polar body.
The following signs indicate that the egg has good potential:
- homogeneous cytoplasm of uniform color;
- lack of granularity of the cytoplasm.
Signs of decreased oocyte quality:
- the presence of vacuoles (sacs filled with fluid in the cytoplasm);
- dark color of the cell;
- presence of inclusions;
- deformation or heterogeneity.
- fatty deposits inside the cytoplasm.
- complete degeneration (Deg)
Such deviations are more common in older reproductive age, although the reasons may be improper nutrition, bad habits, smoking even in the past, endometriosis. Oocyte abnormalities are associated with lower fertilization and embryo quality.
What is the Maturity of Oocyte
Not all oocytes obtained in an IVF program will be mature. An immature egg cannot accept a sperm for fertilization.
Two components are involved in oocyte maturation:
- Nuclear component – includes genetic material (chromosomes / DNA).
- Cytoplasmic component – includes a surrounding fluid called cytoplasm.
Both of these components must mature for fertilization and proper development of the embryo.
The nuclear component of the oocyte matures after the introduction of the ovulation trigger. The trigger instructs the chromosomes to continue meiosis (the chromosomes of the oocyte are separated to prepare for union with the chromosomes of the sperm). The cytoplasm matures as the oocyte’s DNA produces and stores specific factors in the cytoplasmic fluid.
When you hear that an oocyte is mature, it means that the egg has a polar body. An immature oocyte does not have a polar body. The presence of a polar body tells us that the chromosomes have split (one half in the egg, the other half in the polar body). In the nucleus of a mature egg, there should be 23 chromosomes, so the oocyte is ready to unite with 23 chromosomes of the sperm and form the karyotype of a healthy person – 46 chromosomes.
Oocytes that have not reached maturity can have two forms: oocytes in meiotic metaphase I (M1) and germline vesicles (GV).



Embryo Development

Day 0
mature oocyte ready for fertilization
After the puncture of the follicles, the embryologist receives the eggs surrounded by cumulus (granulosa cells). Due to the dense layer of granulosa cells, it is not possible to immediately determine the quality and maturity of the oocyte. Further, depending on the fertilization method, the embryologist either cleans the oocyte from cumulus – this is necessary for IVF.
After cleaning, the state of the oocyte is determined. At the same time, the preparation of the man’s sperm takes place. In the case of using the ICSI method, the embryologist selects the most morphologically correct sperm for fertilization.

Day 1
embryo of the 1st day of development (stage of pronuclei)
18 hours after ICSI, we assess whether fertilization has occurred. Normally, two pronuclei (precursors of the nuclei of future blastomere cells into which the embryo begins to divide) should be determined. With correct fertilization, both pronuclei are clearly visible, they are designated 2PN.
If pronuclei are not detected, then most likely fertilization did not occur (0PN). Sometimes we observe 1 pronucleus (1PN), in which case fertilization has occurred, but such embryos need to be closely monitored, as a rule, they have a reduced cleavage potential. If we observe 3 PN or more, then fertilization has occurred incorrectly (the wrong set of chromosomes is contained).

Day 2
Crushing stage. The embryo consists of 4 cells
At this stage, further cleavage of the embryonic cells occurs. The pronuclei disappear and the embryos begin to divide. The embryonic cell should by now split into two, and these two cells result in a four-cell embryo. Evaluation of the quality of embryos is carried out 40-42 hours after fertilization.

Day 3
embryo of the 3rd day of development (8 cells)
In a healthy embryo, cells continue to divide, gradually increasing their number. Normally, the cleavage of embryonic cells should be symmetrical and uniform (blastomeres of the same size).
Evaluation of the quality of embryos is carried out 72-74 hours after fertilization.

Day 4
morula stage (compaction)
On the fourth day of development, the embryo begins to compact the boundaries of its cells become indistinguishable. The embryo on this day is not evaluated by embryologists due to the low information content of this stage of development.

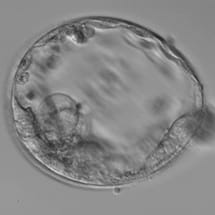
Day 5
blastocyst stage
On days 5-6, ideally 120 hours or more after fertilization, the embryo forms a blastocyst. The blastocyst consists of two populations of cells – the trophoblast (cells of the future placenta) and the inner cell mass (from these cells the fetus will form).
Blastocyst Structure

Embryo Assessment on Early Stages
The choice of the embryo for transfer to the uterine cavity is very important. After fertilization, the embryologist closely monitors the development of embryos, while assessing the development of each of them individually. The main characteristics are the presence of fertilization, the rate of development and the quality of the embryos.
First of all, the embryologist looks at the number of cells.
Normally, on the 2nd day of development, the embryo consists of 2-5 cells, on the 3rd day – from 6-8, and on the 4th day the number of cells is difficult to count, because their fusion begins and the embryo at this stage is usually called morula.
When describing an embryo of 2-3 days of development, a letter is added to the number indicating the number of blastomeres – reflecting the quality and shape (morphology) of the blastomeres themselves, and the presence or absence of fragmentation (separation of non-nuclear non-viable cytoplasmic fragments from the cells).
- A – nuclear-free fragments are absent, blastomeres (embryonic cells) are even, of the same size, have one nucleus, homogeneous cytoplasm;
- B – the number of non-nuclear fragments of the cytoplasm is less than or equal to 25%;
- C – the number of fragments without nuclei ranges from 25 to 50%, there are abnormalities in the size and shape of blastomeres, there are inclusions in the cytoplasm;
- D – more than 50% non-nuclear fragments. This state is called total fragmentation. Such embryos are not used for transfer into the uterine cavity (unless there are no embryos of a different quality and the patient insists on transfer). It must be said that even in such cases, a normal pregnancy can occur, only this probability will be many times lower than when transferring embryos of quality A or B.
Today, when science does not stand still and scientists from all countries share their experience and problems, new ideas for the classification of embryos are being proposed. But one thing in them remains unchanged – this is the digital and letter designation of the number of blastomeres and fragmentation in the early stages of embryonic development, as well as the size of the cavity and the quality of blastocyst cells.
Blastocyst Classification
By the fifth day, the cavitation process begins (a cavity is formed in the embryo, the cells are divided into two groups – trophoblast and internal cell mass (ICM), as a result, on the 5-6th day of development, a blastocyst is formed, which consists of 156-200 cells. hatching), the embryo prepares for implantation to the uterine cavity.
Classification for blastocysts is more complicated than for embryos of earlier stages, and consists in assessing the number and quality of cells in different parts of the blastocyst, the size of the embryonic cavity. This embryo grading system has a correlation between the quality of the transferred embryos and the pregnancy rate.
The Gardner scale is used to classify blastocysts. This scale consists of one number and two capital letters.
The number describes the size of the blastocyst cavity, the first letter is the quality of the inner cell mass, the second letter is the trophoblast (outer cell mass):
- Blastocyst size, volume of its cavity:
- The cavity takes up less than 50% of the blastocyst.
- The cavity occupies 50% of the blastocyst.
- The cavity occupies more than 75% of the blastocyst.
- Blastocyst, the cavity of which is 2 times the internal cell mass.
- Blastocyst in which the shell began to open (hatching occurred)
- Blastocyst completely free of the membrane, ready for implantation.
- Characteristics of the cells from which the fetus will develop (internal cell mass):
- A. There are many cells, the boundaries between cells are indistinguishable.
- B. Cellular shapes are distinguishable, with some minor defects in them (granularity, etc.)
- C. Defects in cells are significant, there are signs of apoptosis (cell death).
- D. Degeneration of cellular composition.
- Characteristics of the cells of the outer cell mass (trophectoderm), which form the future placenta:
- A. There are many cells, they are located in one layer, without defects.
- B. Cell mass is slightly reduced.
- C. There are few cells, there are defects, inclusions.
- D. Degenerative processes.
We Can Evaluate Embryo Quality With A Microscope
Three Value-Points
 |
 |
 |
| 1 embryo size (from 1 to 6) |
2 quality of inner cell mass (ICM) |
3 trophectoderm quality |
Quality of inner cell mass (ICM): assessment from A (good) to C (poor)
 |
 |
 |
| ICM – A good quality inner cell mass |
ICM – B satisfactory quality |
ICM – С poor quality |
Trophectoderm quality (TE) from A (good) to C (poor)
 |
 |
 |
| TE – A good quality |
TE – B satisfactory quality |
TE – C poor quality |
Laser Hatching
An important factor in the onset of pregnancy is the implantation of the embryo, its attachment to the uterine cavity.
For this to happen, the embryo needs to get out of its zona pellucida.
The zona pellucida of the egg also performs two important functions in the future of the embryo: it prevents more than one sperm from entering the egg during fertilization and keeps the cells of the embryo in the process of cleavage.
The natural process of hatching (hatching) occurs on the 5-6th day of embryo development – at the blastocyst stage. If this process does not occur on time, the willingness to accept and carry a pregnancy (implantation window), which lasts only 24 hours, closes and the woman’s body prepares for the renewal of the endometrium (menstruation).
Assisted hatching is the incision of the zona pellucida in order to release the blastocyst for implantation to the uterine wall.
Indications for hatching:
Not a typically thickened shell, or not its correct shape; The woman’s age is over 35;
The need for preimplantation genetic testing (PGT);
Embryos after cryostorage or obtained during fertilization of thawed oocytes;
In the past, there have been unsuccessful attempts at IVF without implantation with good quality of transferred embryos and endometrium.
In our medical center, we use an efficient and completely safe laser system of the latest generation for assisted hatching. This allows you to effectively help the embryo and significantly increase the likelihood of pregnancy.
How is an embryo biopsy performed?
Preimplantation development of the embryo lasts about 7 days from the moment of fertilization of the oocyte with a sperm cell until its implantation into the uterine cavity.
This is a very important period of development and the only one that can be outside the mother’s body, in vitro.
In 7 days, the embryo develops from 1 cell to about 156 cells, differentiation of cells into the internal cell mass (ICM), from which the fetus develops, and trophoblast (cells for the development of the future placenta). The embryo at this stage looks like a vesicle with a diameter of 0.2-0.3 mm and is called a blastocyst.
On the 5-6th day of embryo development, before transfer to the uterine cavity, we have the opportunity to take about 5 trophoblast cells. This is called a trophoblast biopsy, or blastocyst biopsy. The cells obtained from the biopsy of each blastocyst are placed in special labeled tubes and sent to the genetic laboratory.
For an embryo, a biopsy is absolutely safe and does not harm its development. The embryos are frozen (vitrified) until PGT results are obtained.
[embedyt] https://www.youtube.com/watch?v=LGXWUOyfBYY [/embedyt]
Here you can see a video of a blastocyst biopsy. The procedure is performed under an inverted microscope with a magnification of 200x, using glass microinstruments and a laser.
A biopsy is performed for preimplantation genetic testing (PGT) to determine the chromosome set of the PGT-A embryo or to exclude the carriage of monogenic PGT-M diseases, PGT-SR structural rearrangements, which allows a genetically healthy embryo to be transferred and increases the chance of pregnancy.
Embryo mosaicism
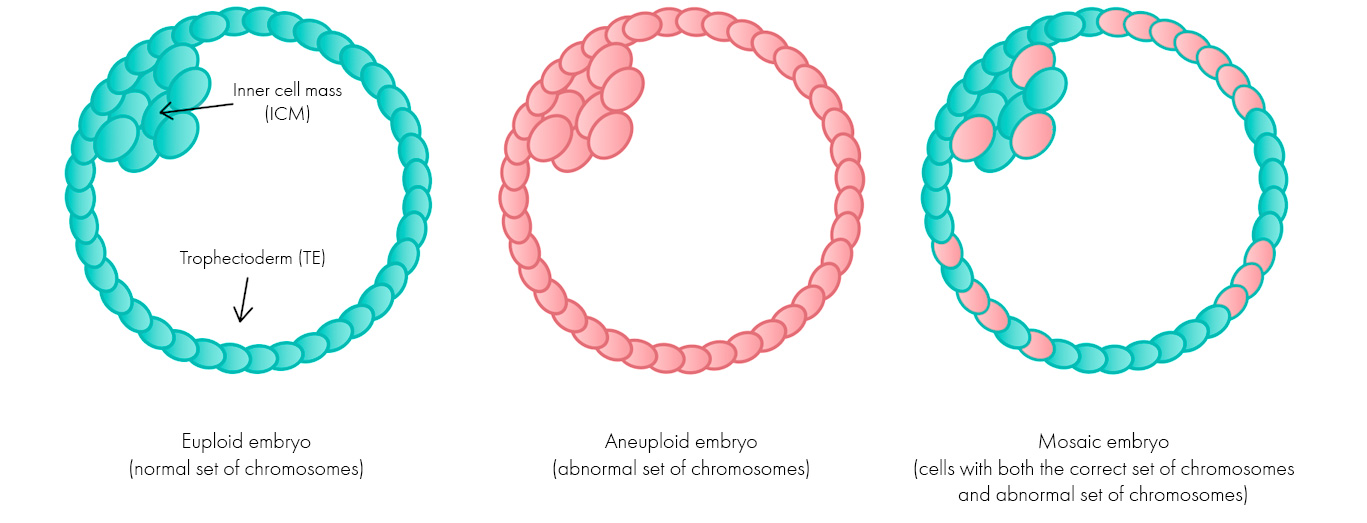
Preimplantation genetic testing of PGT-A embryos made it possible to determine changes in the set of chromosomes. With the introduction of this method, it became clear that along with chromosomally healthy (euploid) embryos and aneuplot embryos, that is, with an incorrect chromosome set, there are also so-called mosaic embryos.
Embryos with chromosomal mosaicism contain two or more cell lines with different numbers of chromosomes (for example, some cells are euploid and others are aneuploid).
The frequency of formation of mosaic embryos is about 18-20% at the blastocyst stage and occurs with the same frequency regardless of age.
Embryos, which are completely aneuploid, arise from errors in the chromosomes in the egg or sperm that are transferred into every cell in the embryo. In mosaic embryos, the error occurs after fertilization, and is only transferred further to cells that already originate from this cell.
It is possible that mosaicism is the result of rapid cell division and relaxation of the “checkpoints” characteristic of early embryonic development, and that this is a transitional phase during development.
Of course, when there are healthy embryos as a result of PGT-A, we consider them as a priority for embryotransfer. However, there are situations when there are no euploid embryos. Then, after assessing the degree of mosaicism, we can transfer the mosaic embryo.
Our embryologists

chief medical officer, leading reproductologist, gynecologist, endocrinologist, MD, PhD. ; main specialty: gynecological endocrinology, treatment of infertility due to premature decline/insufficiency of ovarian function, treatment of embryo implantation disorders.



Obstetrician-gynecologist, endocrinologist, and ultrasound diagnostics specialist. Main specialization: gynecology, endocrinology, leading expert in the clinic in the fields of endocrine gynecology and anti-aging therapy.


Obstetrician-gynecologist and ultrasound diagnostics specialist. Main specialization: endocrine gynecology, pregnancy management, including after IVF, prenatal diagnostics (Fetal Medical Foundation license).


Doctor of Internal Medicine, Dietologist, Allergist, Ultrasound Diagnostics Specialist.

Obstetrician-gynecologist of the highest category, reproductive specialist. Main specialization: gynecological endocrinology — diagnosis and correction of conditions related to PCOS, premenstrual syndrome, ovarian-menstrual cycle disorders, endometriosis, correction of conditions related to different stages of menopause, ovarian cysts. Treatment of all forms of infertility and recurrent pregnancy loss.

Obstetrician-gynecologist, reproductive specialist. Main specialization: gynecology, infertility treatment, endocrine gynecology, pregnancy management (including pregnancy after IVF)

Obstetrician-gynecologist, reproductive specialist, ultrasound diagnostics expert. Main specialization: endocrine gynecology, management of high-risk pregnancies, diagnosis and treatment of all types of infertility, hysteroscopic treatment of uterine diseases
Prices
| Наименование | Стоимость, грн. |
| ICSI ( до 10 яйцеклеток) | 7 700 |
| Культивирование эмбрионов | 6 500 |
| Вспомогательный хетчинг | 3 500 |
| Трофектодермальная биопсия | 3 370 |
| Заморозка (витрификация) эмбрионов с учетом стоимости 1 криотека | 4 180 |
| Дополнительный криотек | 855 |
| Криохранение эмбрионов 1 месяц | 335 |
| Криохранение эмбрионов 3 месяца | 855 |
| Криохранение эмбрионов 6 месяцев | 1 508 |
| Криохранение эмбрионов 12 месяцев | 2 620 |
| Спермограмма | 420 |