

Table of contents
Endometrial hypoplasia is a condition where the uterine lining does not reach the necessary thickness and functionality for successful embryo implantation. This is a serious problem for achieving pregnancy naturally and for treating infertility through IVF. However, modern treatment approaches significantly increase the chances of a successful pregnancy.
Classification of Endometrial Hypoplasia:


Normal endometrium: A healthy endometrium has sufficient thickness and structure for successful embryo implantation.
Pathological endometrium: Thin and disrupted structure that makes it difficult for the embryo to implant
By the level of estradiol circulating in the female body:
- Hypoestrogenic form — insufficient endometrial growth due to low estradiol levels (PCOS, hypogonadism, premature ovarian reserve depletion, menopause).
- Normoestrogenic form — normal estradiol levels, but impaired receptivity (cell sensitivity to estrogen) or circulation (chronic endometritis, autoimmune endometritis, post-infection changes, endometrial trauma from previous interventions — abortion, tumor removal).
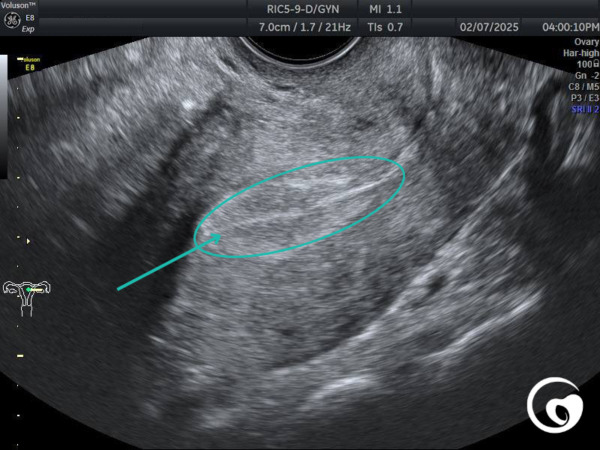
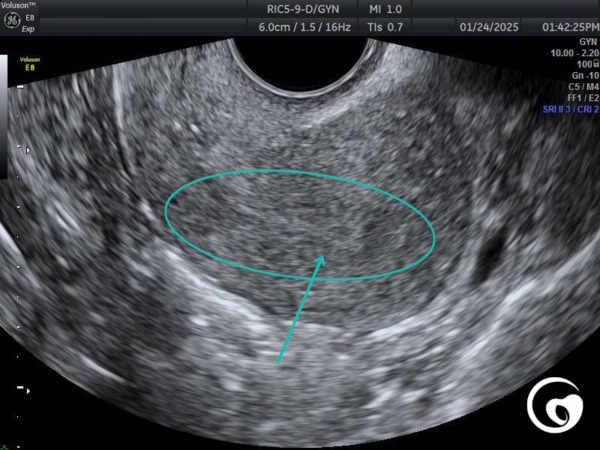
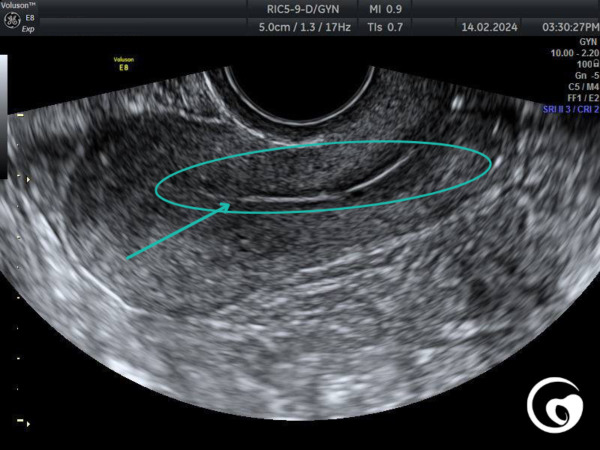
1. By the thickness of the endometrium (based on ultrasound data on the day of ovulation trigger, ovulation, or embryo transfer day):
- Mild hypoplasia — 6.1–7.0 mm
- Moderate hypoplasia — 5.1–6.0 mm
- Severe hypoplasia — <5.0–4.9 mm
2. By morphological features:
- Atrophic endometrium — few glands, poor vascularization (weakened blood supply).
- Fibrous endometrium — presence of adhesions (consequences of infections, curettage).
- Inflammatory endometrium — chronic endometritis or autoimmune endometritis (the body’s immune system attacks its own endometrial cells and destroys them).
Modern Treatment Methods for Endometrial Hypoplasia:
- Chronic endometritis treatment includes anti-inflammatory therapy, antibiotic treatment with mandatory microbiome support, and control 3 weeks after completing the antibiotic course.
- Adhesion process (synechiae of the uterine cavity): 3D ultrasound can clearly visualize this, and hysteroscopy is performed to visualize the state of the endometrium and remove synechiae. After removal, mandatory prevention of their recurrence should be prescribed due to a high risk of relapse.
1. Hormonal therapy:
- Estrogens (Progynova, Estrofen, Divigel, Estrogel) — stimulate endometrial cell growth (proliferative phase).
- Progesterone (Utrogestan, Ingesta, Dufaston) — secretory transformation (progesterone affects endometrial cells only after proper preparation with estrogen).
- Somatotropin (growth hormone) — increases endometrial receptivity and vascularization.
These medications should only be prescribed by a reproductive specialist after a thorough examination and determining the causes and treatment tactics for endometrial hypoplasia.
2. Methods to improve blood supply:
Angioprotectors and vasodilators:
- L-arginine (Tivortin, Tivomax) — 100 ml IV for 5–10 days during the proliferative phase. This amino acid can also be taken orally in a dosage of 1000–2000 mg/day between meals.
- L-citrulline — amino acid that increases nitric oxide levels and improves microcirculation (750–1500 mg/day, also between meals).
- Pentoxifylline (Trental) — 100–200 mg/day.
- Sildenafil (Viagra) — 25 mg 2 times/day vaginally in the first phase of the menstrual cycle.
- Actovegin — 200 mg 2 times/day intravenously or in tablets.
3. Uterine cavity irrigation:
- PRP therapy (platelet-rich plasma). Stimulates blood supply activity and endometrial cell regeneration. Course: 2–3 irrigations with a 5-day interval during the first phase of the menstrual cycle.
- Endometrial irrigation with exosomes — promotes the restoration of the endometrial tissue matrix. Stimulates cell renewal and influences the restoration of endometrial receptor systems.
- Hyaluronic acid — stimulates cellular regeneration.
4. Use of growth factors (VEGF, EGF, IGF-1):
- Used in the form of injections or uterine cavity irrigation during the first phase of the menstrual cycle.
- They help develop blood vessels and improve receptivity. Can only be used after being prescribed by a reproductive specialist with experience in this support method.
5. Nutraceutical support is an additional aid to improve the condition of the female body before implantation:
- Antioxidants and nutraceuticals that improve endometrial condition:
- L-citrulline — stimulates nitric oxide synthesis, improves microcirculation.
- Vitamin B9 (in the form of methafolin) and B12 (in the form of methylcobalamin) for supporting blood vessel walls and building ferritin.
- Vitamin E (tocopherol acetate) is best found in wheat germ oil for adding to food.
- Omega-3 — anti-inflammatory effect, improves blood flow.
- Vitamin D3 (cholecalciferol) — increases endometrial receptivity (at least 2000 IU/day).
- Resveratrol (in the form of trans-resveratrol) — antioxidant, improves vascularization.
- Coenzyme Q10 (ubiquinol) — improves energy exchange in endometrial cells.
- Myo-inositol — 4 g/day corrects insulin resistance and improves endometrial receptivity.
-
Embryo Transfer Preparation in Endometrial Hypoplasia:
1. Selection of endometrial preparation protocol for embryo transfer:
- Protocol with hormonal support (Estrogens + Progesterone).
- Natural cycle (with good levels of own hormones).
- PRP protocol + somatotropin (in complex cases), combined with optimizing blood supply to the endometrium.
2. Endometrial thickness assessment before embryo transfer:
- Minimum thickness of 7 mm before progesterone administration.
- Presence of a trilaminar structure before progesterone support (on days 14–15 of the menstrual cycle).
3. Blood supply assessment:
- Doppler measurement of blood vessels (PI <3).
4. Embryo transfer during a favorable period (endometrial readiness for implantation):
- On days 5–6 after starting progesterone (19–21 days of the menstrual cycle).
5. Post-transfer support:
- Continuation of hormonal support.
- Anticoagulant therapy (especially important with high doses of estrogens, which may thicken the blood and worsen blood supply). Genetic thrombophilia indicators should also be considered, as they can affect blood supply to the endometrium and implantation efficiency.
- Immunotherapy for autoimmune factors.
Conclusion:
Using PRP, exosomes, growth hormone, L-citrulline, and nutraceutical support significantly improves the condition of the endometrium and increases the chances of successful implantation. Our clinic applies the latest approaches to endometrial preparation before embryo transfer. In complex cases, we use autologous (patient’s own) stem cells from the endometrium to stimulate endometrial growth. A comprehensive, individualized approach helps even in the most complex cases to achieve the desired pregnancy.
It should be remembered that the diagnosis of endometrial hypoplasia requires a comprehensive approach and the experience of a reproductive specialist. Endometrial condition is important not only for successful embryo implantation but also for the proper formation of the placenta and pregnancy (to avoid fetal-placental insufficiency). In our clinic, we have accumulated knowledge and experience to successfully help our patients achieve pregnancy and carry the baby to term even in the most complex situations. Schedule a consultation at our clinic to select the optimal endometrial preparation protocol for successful embryo transfer!



