
Table of contents
When we talk about fertility, the focus most often shifts to hormones, eggs, or age. But there is a factor that often remains unnoticed — the structure of the uterus. In clinical practice at Reprolife, we regularly see situations where it is specifically anatomical features that explain what for years looked like “unexplained” infertility or recurrent pregnancy loss.
And it is important to understand: most of these changes are formed even before birth.
How the uterus is formed during embryonic development
The development of the uterus begins as early as the 4th–6th week of intrauterine life. During this period, the Müllerian ducts are formed — structures from which the uterus, fallopian tubes, and the upper part of the vagina will form in the future. Next, a complex process occurs, which includes three key stages: the formation of two ducts, their fusion, and the subsequent “dissolution” of the internal septum to form a single cavity.
This process continues until approximately the 16th week of pregnancy. It is during this period that any influence can change the outcome. Every anomaly is a reflection of the stage at which development was disrupted.
Why congenital features of the uterine structure occur
Causes are divided into 2 groups of factors:
– chemical (hypoxia, malnutrition of the embryo, hormonal disorders, action of toxins);
– biological (viral, bacterial infection)
– genetic;
– changes in germ cells;
Congenital malformations of the genital organs are often combined with changes in the development of other organs and systems: urinary, skeletal, cardiovascular, etc. This is explained by the fact that the cause affects not only the primordia of the genital organs but also the primordia of other organs simultaneously.
How common is it: figures and statistics
In the general population, such features occur in 0.5–6.7% of women. But among patients with reproductive difficulties, these figures are significantly higher:
- about 8% in cases of infertility
- up to 16% in cases of recurrent miscarriage
- up to 24–25% in a combination of these conditions
- This means that every fourth woman with such problems may have an anatomical factor.
What are uterine anomalies and how do they affect fertility?
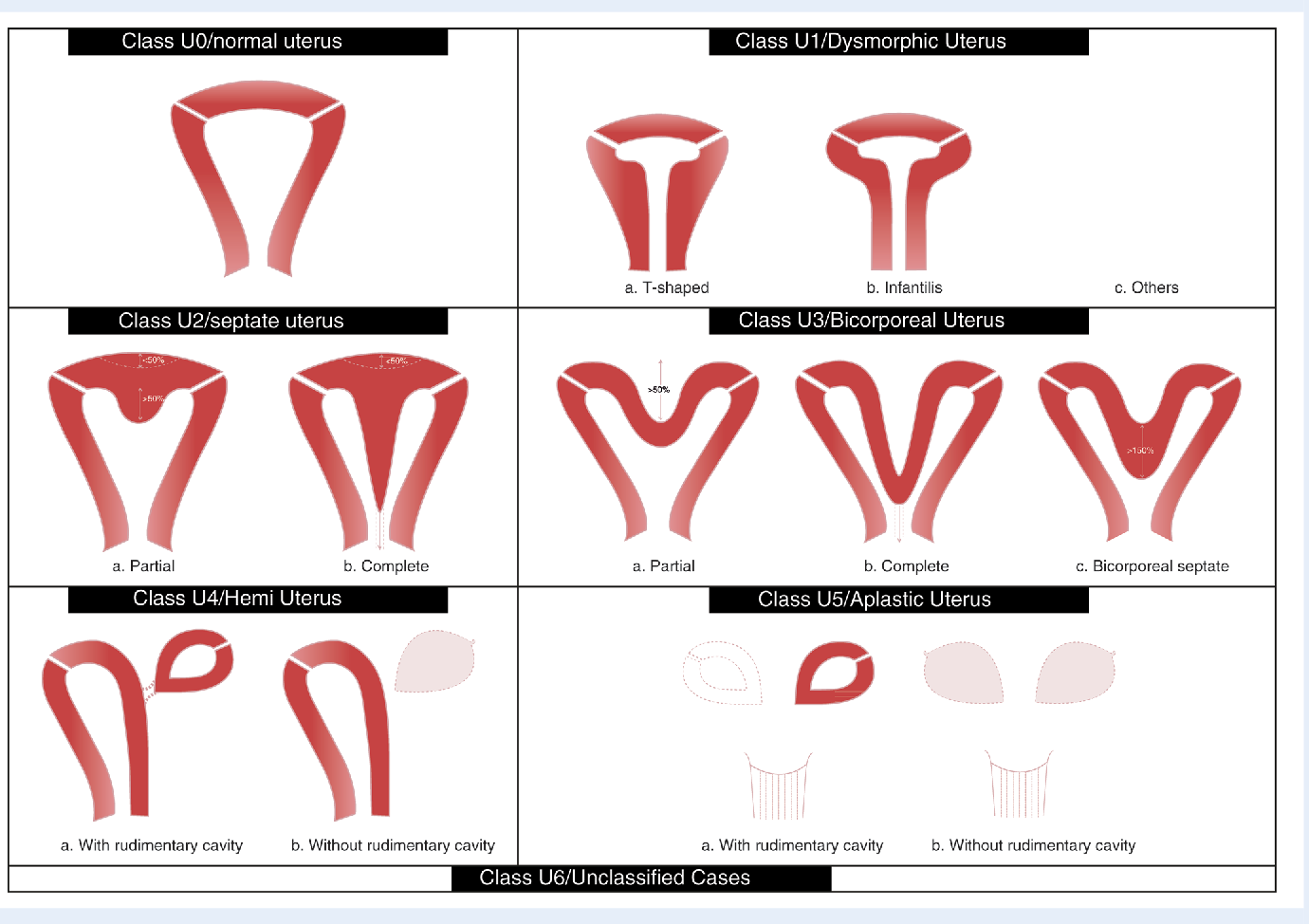
According to the ESHRE / ESGE classification, several types of anomalies exist.
The most common is the intrauterine septum (up to 35–55% of cases). It is most closely associated with miscarriage: the risk of miscarriage can reach 60–80%.
A bicornuate uterus increases the risk of premature birth.
A unicornuate uterus is associated with a high risk of pregnancy complications. Also, with these specific uterine development features, we see a high predisposition to a thin endometrium (endometrial hypoplasia), which specifically complicates embryo attachment.
Rare conditions, such as uterine aplasia, occur in approximately 1 in 4500–5000 women.
Let’s look at specific features of the uterine body structure in more detail.
The intrauterine septum is the most common among atypical uterine structures. Hysteroscopic metroplasty is currently recognized as the “gold standard” for treating women with a uterine septum. Most publications indicate that indications for such surgery are spontaneous miscarriages, premature births, and conception problems when endocrine, infectious, and other possible causes are excluded. That is, if this is an incidental finding during an examination without complaints, this condition does not require any surgical treatment.
What are the symptoms of uterine structure anomalies?
Symptoms may include:
- Absence of menstruation
- Irregular or painful menstruation
- Heavy or prolonged menstruation
- Pelvic pain that may come and go
- Discomfort or pain during sexual intercourse
- Recurrent pregnancy loss or miscarriages
- Infertility or difficulty with pregnancy
- Premature birth or premature rupture of membranes
- Abnormal fetal position during pregnancy
- Symptoms related to urination if there are also kidney problems
Why many women are unaware of this
Diagnosis of uterine anomalies: which methods actually work
Interesting fact: the link to the kidneys
This is why examination of the urinary system is mandatory.
What this means for the possibility of getting pregnant
The presence of an anomaly does not mean that pregnancy is impossible. But it can affect:
embryo implantation,
the course of pregnancy,
the risk of miscarriages or premature births.
And that’s why it’s important not just to “know,” but to understand how this affects your specific situation.
Conclusion
trust in your doctor significantly increase the chances of a successful pregnancy. Every story is unique, and for most women, a happy ending is possible. The main thing is not to be left alone with your fears and questions. Together, we can make the path to your motherhood safe and confident.
Frequently Asked Questions (FAQ)
Can I get pregnant with a uterine anomaly?
Yes, in most cases, pregnancy is possible but requires the right approach.
What is the most common anomaly?
Intrauterine septum — up to 50% of cases.
Is surgery always necessary?
No, only in the presence of clinical indications.
Do I need to check my kidneys?
Yes, up to 30–40% of cases are accompanied by anomalies of the urinary system.
List of Sources Used:
2. https://www.mdpi.com/2077-0383/11/5/1251
3. Obstetrics and Gynecology: National Guide. Vol.4: Operative Gynecology. Edited by Zaporozhan V.M. K.: VSV “Medicine” 2014.




